Clinical diagnostic testing laboratories are under increased pressure to continually provide accurate results for each patient tested while reducing turnaround times (TATs). This becomes increasingly difficult as new tests are introduced to identify new analytes for new disease targets, or new molecular technologies are added to core facilities in an effort to reduce costs, complexities, and overall analysis time over current technologies.
Accurate laboratory results are critical for improving medical diagnoses and ensure patient safety. Many studies have shown that as much as 70% of medical decisions made by clinicians depend upon accurate laboratory results. Yet despite advances in new testing technologies, laboratory automation, and sample tracking software, there are still considerable error rates in clinical diagnostic labs.1
Total turnaround time in laboratory testing has been traditionally characterized as the time from specimen collection to the reporting of results. 2,3 Despite improvements in analytical testing systems (i.e., automation), little to no measurable improvements have been demonstrated for the preanalytical phase of TAT. Efforts to address some aspects of the preanalytical phase, specifically specimen transport (i.e., pneumatic tubes), as well as efforts to streamline laboratory processes (i.e., lean), have had minimal impact on TAT.4
The main issue laboratories have to address is how to decrease TAT and testing costs while reducing testing errors. In the preanalytical steps (the major source of mistakes in laboratory diagnostics), errors arise during patient preparation and sample collection, transport, preparation, and storage.5 The most commonly reported types of preanalytical error6 are:
- Missing sample, sample ID, and/or test request ID
- Erroneous or missing ID
- Inadequate sample (low volume, diluted)
- Incorrect vials/containers
- Contamination from infusion route
- Inappropriate blood-to-anticoagulant ratio
- Incorrect transport and storage conditions
- Hemolysed, clotted, or insufficient quantity.
More than one-fourth of all preanalytical errors are estimated to result in unnecessary investigation or inappropriate patient care, resulting in additional financial burden on the healthcare system.7 On average, preanalytical error costs represent between 0.23% and 1.2% of total hospital operating costs. This unnecessary expenditure can be extrapolated to a typical U.S. hospital with approximately 650 beds to $1.2 million per year.8
Eliminating the centrifugation step in the preanalytical process is key to addressing many of the preanalytical errors that occur and dramatically reducing TAT for routine chemistry and molecular diagnostic tests. Centrifugation errors such as incorrect speed, incorrect or broken tubes, erroneous temperature, and insufficient centrifugation can account for greater than 6% of all preanalytical errors.
A standard blood-collection tube reduces the process time from the recommended 30 minutes of clotting followed by 10 minutes of centrifugation to 5 minutes of clotting followed by as few as 3 minutes of centrifugation. In a study investigating the effects of different centrifugation conditions on clinical chemistry and immunology test results, there was no difference shown in test results between centrifugation at 7 minutes versus 10 minutes. Although these measures may reduce TAT for some tests performed in the laboratory, they do not remove the potential for preanalytical errors, the time to transport the sample to the lab, or the labor to transport or process the sample.
The SerumSTAT collection tube (Figure 1) from SerumDPT Bioscience (pronounced “Serum-dipity”) (Cambridge, MA) eliminates centrifugation in the preanalytical phase. When used in place of a standard blood-collection tube, the SerumSTAT separates serum from whole blood while the blood is being drawn from the patient’s arm into the evacuated, two-chamber tube. The action is totally passive. The device delivers 250 µL of plasma/serum in under 1 minute, completely eliminating the need to transport the samples to the lab for centrifugation prior to clinical testing.
 Figure 1 – SerumSTAT collection tube.
Figure 1 – SerumSTAT collection tube.As shown in Figure 2, the SerumSTAT is designed to work in a similar manner to a standard blood-collection tube. Drawn blood enters a blood-collection chamber that houses a filtering mechanism through a flow restrictor to control the rate of blood entering the chamber. Whole blood separates through the filter and serum or plasma, depending on whether anticoagulant is used, and is collected in the bottom collection tube. After 1 minute, the blood-collection tube is separated from the collection chamber, resulting in 250 µL of serum/plasma. The collection tube is able to control the pressure gradient without the need of an external control or pumping mechanism, resulting in a user-friendly device that can separate whole blood without hemolysis.
 Figure 2 – Diagram of SerumSTAT. Immediate separation from patient’s arm.
Figure 2 – Diagram of SerumSTAT. Immediate separation from patient’s arm.The SerumSTAT collector has been clinically validated in applications including clinical chemistry, field-based veterinary (bovine) diagnostics, and cell-free DNA testing. In each application, the device was compared to the current standard of care. In each clinical trial evaluation, results from blood collected in the SerumSTAT collector were comparable to results from the current standard.
Results of a clinical chemistry test panel, performed in collaboration with Boston University, are shown in Figure 3. Blood was drawn from 13 patients directly into SerumSTAT collectors and simultaneously into standard blood-collection tubes. All collectors contained heparin as anticoagulant. While results for all chemistry tests performed with samples from either a standard blood-collection tube or the SerumSTAT device showed equivalent results for all standard chemistry tests performed, albumin (ALB) showed disparate results. These were attributed to a lab processing error; as in previous result comparisons, ALB results showed excellent correlation. A larger study currently being conducted in collaboration with Boston University will include a larger sample cohort with multiple replicates to enable a more robust statistical evaluation of SerumSTAT performance.
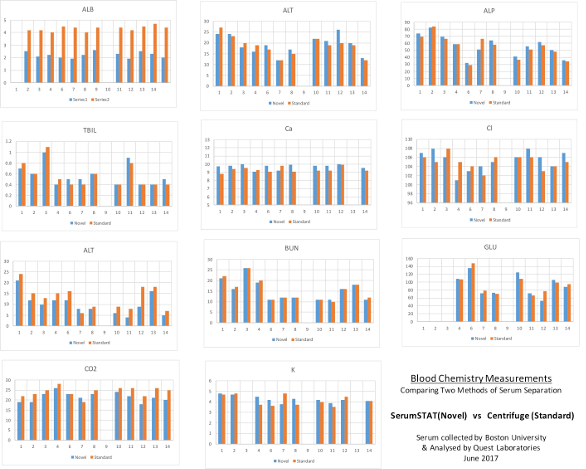 Figure 3 – Results of blood chemistry tests. Comparison of results for standard chemistry.
Figure 3 – Results of blood chemistry tests. Comparison of results for standard chemistry.The SerumSTAT device reduces the TAT or the time for the physician to receive the results by 50 minutes. This estimate includes transport of samples to the lab, clotting time, and centrifugation time.
The ability to remove centrifugation from the preanalytical process not only provides a suitable plasma/serum sample for analysis, while dramatically reducing turnaround time and potentially preanalytical errors, but also enables improved sample stability analysis. Elimination of the centrifuge step also allows sample collection in environments and applications that were previously out of reach.
References
- www.hida.org/app_themes/member/docs/resources/hida_impact-ofdiagnostics-on-healthcare-outcomes.pdf. Accessed July 13, 2015.
- Lippi, G.; Salvagna, G.L. et al. Preparation of quality sample: effect of centrifugation time on stat clinical chemistry testing. Lab. Med. 2007, 38, 172–6.
- Fernandes, C.; Worster, A. et al. Root cause analysis of laboratory turnaround times for patients in the emergency department. Can. J. Emerg. Med. 2004, 6, 116–22.
- Hawkins, R.C. Laboratory turnaround time. Clin. Biochem. 2007, 28, 179–93.
- Lippi, G.; Chance, J.J. et al. Preanalytical quality improvement: from dream to reality. Clin. Chem. Lab. Med. 2011, 49, 1113–26. [PubMed]
- Carraro, P. and Plebani, M. Errors in a stat laboratory: types and frequency 10 years later. Clin. Chem. 2007, 53, 1338–42. [PubMed]
- Plebani, M. and Carraro, P. Mistakes in a stat laboratory: types and frequency. Clin. Chem. 1997, 43(8), 1348–51.
- Green, S.F. The cost of poor blood specimen quality and errors in preanalytical processes. Clin. Biochem. 2013, 46(13), 1175–9.
Darren Lee, M.S., is chief marketing officer, SerumDPT Inc., 104 Lake View Ave., Cambridge, MA 02138, U.S.A.; e-mail: [email protected]; www.serumdpt.com